

Introduction: Acalabrutinib is an irreversible BTK inhibitor (BTKi) in the treatment of relapsed patients (pts) with mantle cell lymphoma (MCL). We and others have previously reported that ibrutinib resistant MCL have poor outcomes and BTK mutations are uncommon in ibrutinib resistant MCL. However, the outcomes, causes of discontinuation, management and mutational landscape in MCL pts who discontinued acalabrutinib are not described.
Methods: We reviewed charts from all relapsed MCL pts treated with acalabrutinib (n=26) in the relapsed setting and identified 21 pts who discontinued acalabrutinib, described in this analysis. Outcomes and management of patients after discontinuing acalabrutinib are reported. Whole-exome sequencing (WES) with SureSelect Human All Exon V6 was performed in 9 pts who progressed on acalabrutinib (10 tumor specimens and 5 matched germline samples); among these pts, 4 tumors were collected before acalabrutinib and 6 were collected after progression on acalabrutinib. One patient had paired sample at both time points (baseline and progression).
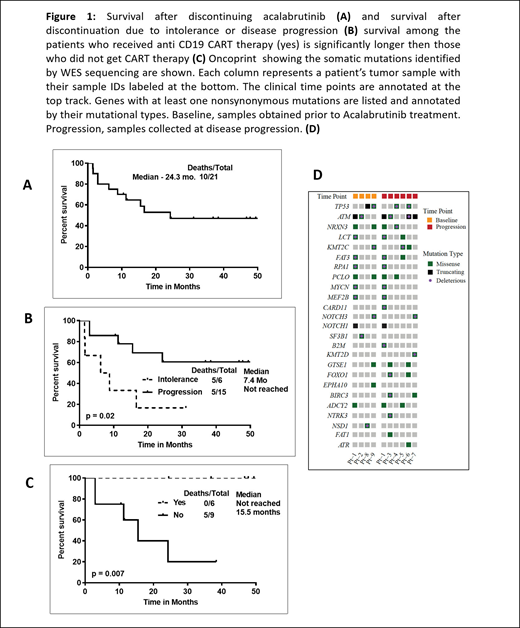
Results: Among the 21 pts who discontinued acalabrutinib, 15 (71%) discontinued due to disease progression (2 pts transformed from classic to pleomorphic MCL at progression) and 6 discontinued due to intolerance (one for fatigue and idiopathic encephalopathy, one due to unrelated severe aortic stenosis, 2 others due to therapy related myelodysplasia and 2 due to cardiac issues). Two pts with cardiac issues had pre-existing coronary artery disease and one of them developed new onset atrial fibrillation. Overall, the median number of prior treatments was 2 (range, 1-3); all had prior chemo-immunotherapy and none with ibrutinib. The median duration on treatment with acalabrutinib was 8.3 months (1 to 50 months) and the median number of cycles of acalabrutinib treatment was 8 (range, 1-53). Thirteen pts had complete remission (CR) as their best response on acalabrutinib, 5 were primary refractory and 3 achieved partial remission. At the time of starting acalabrutinib, 12 pts had classic and 9 pts had blastoid (n=6) or pleomorphic (n=3) features, the median Ki-67 expression was 50% (range, 10-100). Pts who progressed, received acalabrutinib for a median duration of 8.3 months (range, 1-50) while those with intolerance, received acalabrutinib for a median duration of 9.4 months (range, 4-31). Median follow up after discontinuation was 38 months and the median post acalabrutinib survival was 24 months (not reached for progression and 7.4 months for intolerance; p =0.02, Figure-1A-B). Patients who discontinued due to intolerance could not get subsequent treatment for MCL. Among the 15 pts who progressed on acalabrutinib, 14 pts received systemic therapies for MCL [eight received ibrutinib based therapies (4 non responders, 3 achieved CR and 1 were PR and all pts progressed subsequently), 5 got chemo-immunotherapy, bortezomib, lenalidomide and progressed and one pt did not receive any treatment and was lost to follow up and died. Among the 15 pts who progressed on acalabrutinib, 6 patients who received anti-CD19 CAR-T therapy had significantly longer survival compared to those who did not get CART therapy; p = 0.007, Figure-1C. For all pts, at the time of last follow up, 10 pts were alive and in remission under follow up while 11 were dead.
Recurrently mutated genes in these tumors included ATM (6/10; 60%), TP53 (4/10; 40%), KMT2C (3/10), MYCN (2/10), NOTCH1 (2/10), NOTCH3 (2/10), and MEF2B (2/10) (1-D). We did not detect any mutation or copy number alterations in BTK, PLCG2, TRAF2/3 and MYD88 that have been reported previously to be associated with ibrutinib resistance. To investigate the mutation evolution on acalabrutinib treatment, mutation profiles, particularly the mutation variant allelic fractions (VAFs), were compared between the baseline and progression samples from one patient. Mutation of MYCN, MEF2B, ATM, and NOTCH1 were identified in both tumors at similar VAFs, whereas mutation of CARD11 (two mutations), NLRC5 and B2M were detected only at progression.
Conclusions: Relapsed MCL pts who fail acalabrutinib have poor outcomes. Advent of CART therapy has significantly improved survival of these heavily refractory pts. In this small cohort, we did not observe BTK mutations associated with acalabrutinib resistance in MCL pts. Further studies are ongoing to determine acalabrutinib resistance mechanism in MCL.
Lee:Takeda: Research Funding; Aptitude Health: Speakers Bureau; Bristol-Myers Squibb: Consultancy, Research Funding; Seattle Genetics: Research Funding; Oncternal Therapeutics: Research Funding; Guidepoint Blogal: Consultancy; Celgene: Research Funding. Westin:Astra Zeneca: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; Morphosys: Consultancy, Research Funding; BMS: Consultancy, Research Funding; Amgen: Consultancy; Kite: Consultancy, Research Funding; Genentech: Consultancy, Research Funding; Curis: Consultancy, Research Funding; Janssen: Consultancy, Research Funding; 47: Research Funding. Nastoupil:LAM Therapeutics: Research Funding; TG Therapeutics: Honoraria, Research Funding; Merck: Research Funding; Novartis: Honoraria, Research Funding; Gilead/KITE: Honoraria; Gamida Cell: Honoraria; Bayer: Honoraria; Genentech, Inc.: Honoraria, Research Funding; Celgene: Honoraria, Research Funding; Karus Therapeutics: Research Funding; Janssen: Honoraria, Research Funding; Pfizer: Honoraria, Research Funding. Vega:NCI: Research Funding. Flowers:Denovo Biopharma: Consultancy; Genentech, Inc./F. Hoffmann-La Roche Ltd: Consultancy, Research Funding; Pharmacyclics/Janssen: Consultancy; Celgene: Consultancy, Research Funding; Leukemia and Lymphoma Society: Membership on an entity's Board of Directors or advisory committees; TG Therapeutics: Research Funding; Bayer: Consultancy; Eastern Cooperative Oncology Group: Research Funding; AbbVie: Consultancy, Research Funding; Millennium/Takeda: Consultancy, Research Funding; Kite: Research Funding; Spectrum: Consultancy; National Cancer Institute: Research Funding; V Foundation: Research Funding; Cancer Prevention and Research Institute of Texas: Research Funding; Burroughs Wellcome Fund: Research Funding; Karyopharm: Consultancy; OptumRx: Consultancy; Gilead: Consultancy, Research Funding; BeiGene: Consultancy; Acerta: Research Funding. Wang:AstraZeneca: Consultancy, Honoraria, Other: Travel, accommodation, expenses, Research Funding; Nobel Insights: Consultancy; Celgene: Consultancy, Other: Travel, accommodation, expenses, Research Funding; Janssen: Consultancy, Honoraria, Other: Travel, accommodation, expenses, Research Funding; VelosBio: Research Funding; Pharmacyclics: Consultancy, Honoraria, Other: Travel, accommodation, expenses, Research Funding; MoreHealth: Consultancy; Oncternal: Consultancy, Research Funding; Molecular Templates: Research Funding; Beijing Medical Award Foundation: Honoraria; OncLive: Honoraria; Dava Oncology: Honoraria; Verastem: Research Funding; Guidepoint Global: Consultancy; Lu Daopei Medical Group: Honoraria; InnoCare: Consultancy; Acerta Pharma: Research Funding; BioInvent: Research Funding; Juno: Consultancy, Research Funding; Kite Pharma: Consultancy, Other: Travel, accommodation, expenses, Research Funding; Pulse Biosciences: Consultancy; Loxo Oncology: Consultancy, Research Funding; Targeted Oncology: Honoraria; OMI: Honoraria, Other: Travel, accommodation, expenses.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal